
Bodies for Science


An Era of Science over Patients
Johns Hopkins Urologist, Hugh Hampton Young, was pioneering genital reconstruction in the 1930s as Howard Jones was working towards a medical degree. In 1948 Jones and his physician wife Georgeanna became part-time faculty in the school of medicine’s gynecology and obstetrics department.
Post-World War II was an ambitious time for the sciences. Gathered on the Johns Hopkins medical campus (JHM as it came to be later known) in the middle 20th Century were professionals who dabbled in it all. Gender theory were on the brink of going big as the toolbox of the mental health professionals expanded with Freudian psychoanalysis, pharmaceutical concoctions, and diagnostic classifications. So too were the fields of cancer, vaccines, virology, intersex, in vitro fertilization (IVF), and genetics on the brink of great discoveries. Great discoveries though were not always well understood and sometimes sought at the neglect of the patients served and humanity itself.
Four Patients, Four Different Diagnoses, One Doctor
Four history changing patients have received care from the esteemed gynecologist, turned gender surgeon, and later turned IVF expert, Doctor Howard Jones. Each sought care for wildly different conditions. Their impact on the world continues to reverberate to this day.
Three met Jones on the grounds of Johns Hopkins. One was a woman diagnosed with cervical cancer. One was a man with a novel mental condition, “gender identity disorder,” that fell under “psychosexual disorders” in psychiatry’s first bible (DSM-1, 1952). The other was a baby with a circumcision gone wrong. The fourth patient was a woman who sought the Joneses help to conceive at the 1st IVF clinic in the country, the Jones Institute for Reproductive Medicine at Eastern Virginia Medical School that opened in 1980. The Joneses prior IVF work at JHM had been left behind due to a then required retirement age.

All four patients could not have been more unalike, and Jones touched them all. Certainly other physicians were part of the care teams of each but Jones as a gynecologist, gender surgeon, and later IVF expert was unique among them. In chronological order of becoming a patient of the doctor, they are:
Henrietta Lacks; 1920-1951; Lacks, a black woman was diagnosed with cervical cancer by Jones in 1951. She died of the disease after radium treatment the same year.
Phyllis Avon Wilson (birth name unknown); 1929-1989; Wilson, a black man, was the first man to receive sex reassignment surgery (SRS) at JHM. Jones performed his surgery in 1965.
Bruce Reimer (later “Brenda” and then David); 1965-2004; Reimer was the first non-intersex child professionals attempted to “transition” to the opposite sex. Jones performed a bilateral orchiectomy (testicle removal) on baby Bruce in 1967.
Judith Carr; Carr sought IVF services through Jones. In 1981 she gave birth to Elizabeth Jordan Carr, the first IVF baby born on US soil.
It was the common thread of Howard Jones and JHM that stood out as I researched this history. The stories of David Reimer and Elizabeth Carr are told in “Identity Capture and Family Creation.”
It came as no surprise that Jones was the surgeon responsible for cutting into the flesh of the first man to “transition” at JHM. That he was involved with the first US IVF baby sheds light on what the future holds for gender’s victims. But I also recognized Jones’ name from a book I read years ago, The Immortal Life of Henrietta Lacks (2010) by Rebecca Skloot.
Henrietta Lacks is the woman now famous for the cancerous cells taken (not offered) to science. Howard Jones was the doctor who diagnosed her with cervical cancer. It was her cells that produced the first immortal cancerous cell line (HeLa). I pulled that book off my shelf and with fresh eyes from both experiencing and researching the horrors of gender medicine, I reread it. It is the tale of what can happen when a family tragedy turns into industry wealth. It is also a tale about scientific theories that go unchecked while notoriety, achievement, and political agendas outpace the truth.
This post and the following covers an unsettling perspective on the state of medicine in light of Henrietta Lacks and Phyllis Avon Wilson, the first 2 of Jones 4 patients, that could only be told with the passage of time. I am left wondering about the connections between an industry, the patients it serves, and the future ahead.
Gender Rising
In 1966 Jones, psychologist John Money, and a couple of plastic surgeons co-founded the Gender Identity Clinic. It was the first sex reassignment surgery (SRS) center in the US, although other places were also dabbling. Funding came from the transsexual led Erikson Educational Foundation. “Gender” over sex got a foothold in America. More than a dozen other clinics followed suit. Served were intersex patients with biological anomalies but also patients with mental distress. The latter condition was given a name, “gender identity disorder,” despite the lack of agreement it was an independent condition at all.
Years later psychiatrist Jon Meyer would find “gender” patients “familiar” to his distraught mental patients. It was to come to an end in 1979 when the clinic closed. Instead the toxic theories had grown legs and settled in the psyches of ambitious scientists, organizations, and distraught patients. It never died. It hid. Almost 40 years later in 2017 Johns Hopkins Medicine (JHM) reopened a clinic, the Center for Transgender and Gender Expansive Health. “Transsexual” was repackaged as “transgender.” Already subjective gatekeeping whittled away. Patient age wound downward. Sex ratio shifted. The system was rebranded, but it rhymes. “Gender” over sex thrives. There remains no consensus.

Every single thing about “gender” is a lie. The research. The science. The programs. All of it. As the churn of outcry grows it is no longer met with silence but with initiatives to stem the bleeding. The bleeding though remains at a hemorrhage. Toxic theories infest every nook and cranny of society. While cheers of ending childhood “transition” ring out, an adult synthetic sex program thrives, services for drugs and mental health remain plentiful, even for minors, and trans refuge initiatives are underway. Is sanitation of gender theory possible when an adult transgender population has been whipped into existence and society sits on the brink of transhumanism?
Agendas and Narratives
This post is written with skepticism around the field of medicine today. Real conditions, diseases, diagnoses, and treatments do exist. Good medical professionals might be found. This post is not about that. For years and years not a single healthcare provider told my daughter the truth. Not a single one told her the reflection in the mirror was worthy, that flesh and blood does not lie, that injecting testosterone sickens, or that breasts are integral to human females. Industry, all of it, lost me the day she began believing in gender theory. It lost her the day she stopped believing.
It was the HeLa cell line that ushered in a new era in the fields of vaccine, cancer, virology, and genetics. I have no background to evaluate that science, but I can review the information since written about these things. The focus here will be the relevance to the evolving pseudo-scientific agenda of “gender,” a field so completely smoke and mirrors it is unbelievable. How Jones’s myriad collection of patients and diagnoses intersect with science, race, gender, culture, and the future shines insight into the darkness.
Today claims of novel viruses, new vaccines (a moonshot for cancer included), ending HIV/AIDS (forever), and more play out in a cycle of fear, science, and relief, over and over. The science might be foreign to the average citizen. Anyone though can juxtapose those things with “transwoman are women,” “dead daughter or live son,” “boy brain in a girl body,” “uterus-haver,” or the other nonsense spewing from the wizards of science today and an unease settles in. There is no science at all. Do they really want humanity to take any narratives proposed or remedies offered seriously when the same institutions offer synthetic sex services?
As the reality of the sexes is poisoned by the wizards of science, artificial reproductive technologies (ART), already fraught with ethical implications, only multiplies. Children by the millions have now been born via ART. Hundreds of thousands of US youth now identify as “transgender”. Synthetic sex markets feed ART markets. Markets offer possibilities never before brought to fruition. More are on the horizon.
The 2021 documentary, Medical Racism: The New Apartheid, tells the dark history of medical harms and experimentation on African American and Latino communities with vaccines, diseases, abortion and other initiatives. From the unpleasant beginnings of modern gynecology to the exposure of the Tuskegee syphilis study that ran from 1932-1972 causing death and transmission of a treatable condition, medical racism rattles on.
The story goes that both AIDS and COVID are novel viruses requiring novel treatments. In both instances racial minorities have been documented as disproportionately affected. Serious Adverse Events by Celia Farber and others have exposed different perspectives from mainstream narratives. Light now shines on the harms and connections between these novel agendas and between narrative, truth, belief, fear, and industry.
AIDS bred an industry, hundreds of NGOs, and a rallying populace in support of a lifestyle. Pivoting from sexual orientation, to sexual orientation and gender identity, was then easy. SOGI, a new acronym is born. A population believes. The narrative says “affirmation” or death are the only choices. A synthetic sex industry thrives.
The synthetic sex industry that was supposed to end in the 70s has been cultivated into a burgeoning industry today. No longer are a handful of mostly men being ushered through “transitions” but younger patients, both male and female, often with no history of gender identity disorder (today called “gender dysphoria” per psychiatry’s latest bible (DSM-5)) are ushered through drastic procedures at record speeds and great numbers.
“Gender” is not a virus found under a microscope, engineered or not. It is a socially engineered narrative spreading through cultural programming, educational initiatives, and social media. Would drag enjoy the notoriety it now does, and would it have been pushed on US children were it not for the support of a medical industry? Readers will discover in a future post the ties between an industry, race, and drag.
Patients Henrietta Lacks and Phyllis Avon Wilson
Both Henrietta Lacks and Phyllis Avon Wilson were racial minorities who incurred injustices at the hands of a system intent on scientific endeavors. Lacks did not live long enough to comprehend any of it. She instead became sicker and sicker by the day until dying in a hospital room. Little is known of Wilson’s life, but it is easy to imagine he enjoyed the pain he suffered for the spotlight he gained from surgical “transition.” No amount of enjoyment makes gender medicine safe, effective, or ethical.
Henrietta’s family lived the price of unfettered experimentation and Skloot adeptly tells that story weaving the tale of science in and out of a family’s struggle. Visits to Henrietta’s rural home in VA, the support of her family, the love for her children, and references to her painted toenails bring to life a woman whose failing body was used to further science. The contrast of rural life to the industrial town of Baltimore where minorities migrated for employment, and between an expert class and the populace it serves, are striking.
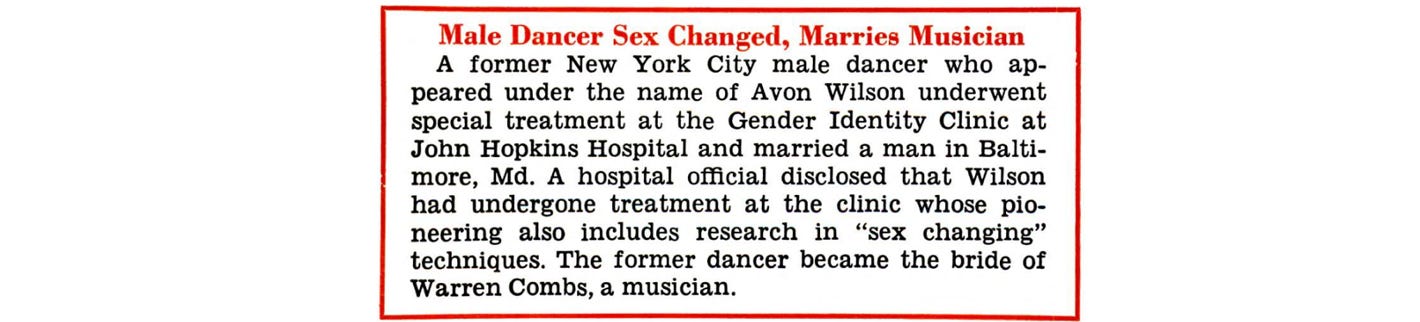
Phyllis Avon Wilson’s life is more obscure. Reports are that an article describing a NY dancer as a “stunning girl” who underwent SRS forced the clinic into the spotlight. This was no girl at all, but Wilson himself. The New York Times was chosen to report the announcement JHM now felt pressure to expose. The short piece was published as front-page news on November 21, 1966.
Color(Race) and SOGI Markets
Johns Hopkins was established in the late 19th Century by a wealthy businessman to serve all people “regardless of age, sex, or color” at a time when segregation was law and few hospitals treated blacks. The differential treatment offered those on the wrong side of segregation though remained.
It is unknown whether Henrietta’s diagnosis came too late despite an earlier appointment but her treatment was endured in the “colored” wards and her lifeless body was stored in the “colored freezer.” A chapter called “Night Doctors” describes the fear instilled in a population, some fictitious, some factual.
Henrietta’s family fared no better when they began to learn details of their loved one whose cells had been transported around the world to the tune of billions of dollars. Healthcare struggles were endured, the truth was hard to find, finances were tight, explanations were thin, and no money or recognition was forthcoming. Samples were taken from surviving family members. A benefit to them they believed was to benefit science, again. Miscommunication and misunderstanding were abundant.
Today alongside age, sex, and color (now race) are sexual orientation and gender identity (SOGI) in JHM’s policy statement. The fictitious notion of “gender” has been treated as a civil rights cause in the modern medical system. A new minority class has been bred and with that recognition can also come mistreatment. For the synthetic sex industry, built on lies, mistreatment is the only option.
Few candidates met the subjective criteria for surgery in JHM’s early gender clinic. It is reported there were about 30 “transitions” in the 13 years it was open. Most patients were male, selected if they might pass as female, and were in relationships with males. In other words they potentially fit the mold of a heterosexual female despite being sexually attracted to men. In 2017 after less than 2 years of the new clinic opening reports claimed there had been 1,400 patients served and more than 300 surgeries performed. The old cohort bears little resemblance with a younger and more diverse sex ratio today. The new clinic remains open for business.
There is scant information of Wilson’s treatment at JHU, whether race played a role in green lighting his “transition,” or much about his life at all except that he was a NY dancer and married a Baltimore musician. It is true though that there is a history of drag in racial minority cultures and that racial minority adult males (particularly Latino ones) comprise a significant percentage of synthetic sex identities today. It is also true that although segregation mostly ended at JHM by the late 50s, the psychiatry department would not begin to follow suit until the late 1960s well after the passage of 1964 Civil Rights Act.
Markets, Markets, Markets
The medical director of JHM’s modern synthetic sex program, Dr. Fan Liang, and countless others, are found in rainbow provider directories covered in other posts. Staying true to the rising social determinants of health model (SDOH) of services blows every patient into commodities to bill and build bigger markets. SOGI is a significant one. Synthetic sex services, cancer treatments, fertility treatment, gender affirming voice treatment, and tissue engineering are among markets serving this cohort. A few markets are discussed.
From Cervical Cancer to Trans Cancer and More
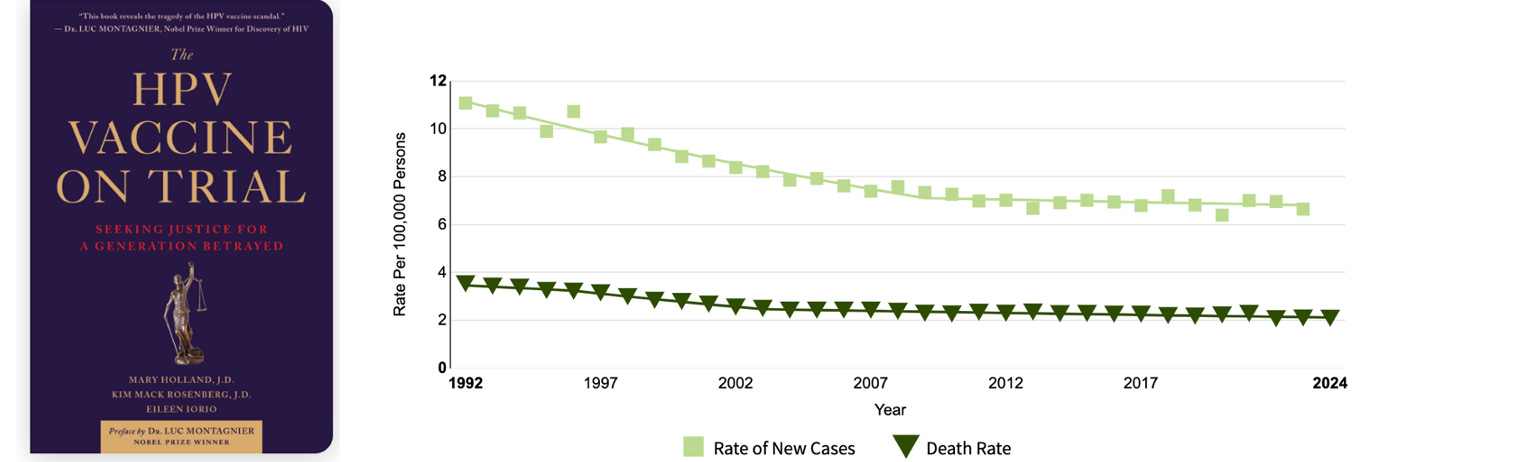
Long after Henrietta’s death in the 80s it was discovered that HeLa cells contained a strain of the human papillomavirus (HPV) that causes cancer. Today radium, known to be toxic and cause secondary cancers, is long gone as treatment for cervical cancer. Diagnoses have declined, and survival rates have increased. In 2006 an HPV vaccine was approved. Diagnoses and death rates had been trending downward long before 2006. The vaccine is advertised as the first cancer preventive vaccine. Within weeks of inoculations serious adverse events were reported to the FDA including deaths. The HPV vaccine held the position of the most dangerous vaccine on the market until the recent injection campaign. HPV Vaccine on Trial tells that history. A video and article provide insights. A 2023 article by Johns Hopkins Bloomberg School of Public health, Do I Need an HPV Vaccine? does not mention the serious adverse events, the deaths, or these trends. Most parents will not receive both perspectives before injecting their children.
If cancer were taken seriously a new field of research and programs for the part of the SOGI market taking on synthetic sex identities would not be. Instead a field around “trans” cancer exists and is growing. Cervical cancer rates do not appear to increase for female to male (FTM) patients, but many types of cancer do for both sexes who succumb to gender’s lies. A non-exhaustive list of possible cancers includes breast (male to female (MTF)), neuroendocrine (MTF), colorectal (MTF), liver (FTM), and potential reproductive cancers (MTF and FTM).
Creating an industry around this new cohort is a focus today. In 2005 the LGBT Cancer Project launched. Like another badge of pride, it is also called “Out with Cancer.” SOGI cancer patients can be matched to clinical trials on their website.
In 2007 a rainbow social worker got in on the cancer game. A woman attracted to females launched the LGBTIQA+ Cancer Network. The current executive director is an FTM patient herself. In the networks own words:

The ever-burgeoning cancer centers also cater to this latest windfall. Memorial Sloan Kettering Cancer Center launched the LGBTQI+ Cancer Care Program in 2013. Langone’s Perlmutter Cancer Center launched LGBTQ+ Cancer Care and Research Program in 2020. It was started when “research” informed the need, not just at Perlmutter, but across all cancer centers. This center is one of 45 National Cancer Institute designated Comprehensive Cancer Centers. These centers are part of Nixon’s 1971 “war in cancer” when he signed the National Cancer Act. The Perlmutter program is headed by a member of the LGBTQ+ brigade. Of course. Enough SOGI identified professionals exist to fill countless positions across industry.
Cervical cancer screening in “transgender men” is encouraged as it is for all women. It is also being studied like the nascent minority group it is not. “Transgender men” are of course just a fiction of modern scientism. The studies are about how to make hairy females who inject testosterone comfortable about uncomfortable procedures for all women. Synthetic sex trumps all. Cancer is relegated to an iatrogenic side effect.
The Business of Body Parts
(Author’s note: This post is already long. Readers might see the coming sections as a post of its own soon.)
The things left behind in surgery or death receive much attention in Skloot’s book. As science speeds ahead in biosynthetic markets this issue is more concerning than it was in the 1950s. Today the sales pitch is in removal and replacement markets.
Consider that Mount Sinai SRS surgeon Miroslav Djordevic is recruiting for cadavers for penile transplantation to female cadavers. The goal is to transplant a cadaver penis on a living female and potentially a live male/ female organ swap one day. Successes in this field could enable MTFs to one day conceive according to the doctor.
The removal of healthy breasts is the number one synthetic sex surgery performed in the US. A network of almost 1,000 U.S. surgeons actively advertise for “top surgery.”
Breast tissue is routinely sent for pathologic assessment. Today the effects of cross-sex hormones and cancer are studied on FTM breast tissue. While tissue banks might not accept tissue from the FTM cohort, in 2014 the UK Breast Cancer Tissue Bank (opened in 2012) funded a study about adding “value” to their tissue bank with an FTM cohort. Authors were affiliated with the London based Barts Cancer Institute and a few UK universities. This group has since folded into Breast Cancer Now. Reports are that all tissue previously collected is now in a central location and available for research. At the bottom of this study is the message that it contributes to the UN Sustainable Development Goal #3 (good health and well-being). This is modern medicine at its finest.
While to date there appears no biobank that collects FTM breast tissue samples in the US, there are institutions that collect and study it. A few examples are discussed. Know there are many others.
An effort to establish a US cohort of FTM breast tissue was made by Harvard’s Beth Israel Deaconess Medical Center from 2013-2018. Using their own patients only one sex-confused female existed in 2013. By 2018 there were 112 bringing the total to 340 in 5 years. The medium age was 25. It is not sudden vaccine harms or atrazine that can swiftly grow this population as some claim. Those things might help but it is business prospects and social engineering at its core. In 2020 the hospital went on to launch it’s Gender-Affirming Services program.
As the saying goes, "Build it and they will come.” It is what Hopkins did in the 60s. Within weeks, “…we got about 3,000 letters from all over America from transsexual patients,” explained a doctor once part of that clinic.

A 2023 study titled “The molecular Consequences of Androgen Activity in Human Breast” begins, “Transgender men are recorded as female at birth but identify as male and may undergo gender-affirming androgen therapy…” That is enough to know the study is garbage despite the fact it is supported by multiple countries, the NIH, and the Department of Defense.
Evaluating the study researchers is more insightful. Researchers include Edward C. Ray, the Cedars-Sinai surgeon who removed or operated on the breasts of the female participants. “Fresh human breast tissue” was taken from 9 “transgender men” ages 18 to 36 and 9 “cisgender woman” ages 28 to 62. Ray leads the first comprehensive academic transgender surgery program in southern California. Ray also does not know what a woman is.
Another researcher, Simon R. V. Knotts, is a founder of Faeth Therapeutics. Faeth was just bought out by Sensei Biotherapeutics, a firm making use of 200 million in investments towards a new drug to “fight cancer with metabolism.” A point worth considering is that removing breasts does not increase metabolism. Testosterone use does.
And then there is the researcher who founded Havah Therapeutics. Havah is working on androgen therapies for breast cancer. A statement on Havah’s website about helping patients with “unnecessary surgeries” and “feelings of reduced femininity and sexuality” is quite a juxtaposition to participation in research on women whose breasts have been lopped off for lies.
A 2025 study called Breast Cancer in a Transgender Man has an astounding conflict of interest statement. One researcher is linked to no fewer than 6 pharmaceutical manufacturers. Another is linked to the organization that guides the synthetic sex industry itself, WPATH.

Study researchers used the Gender Preoccupation and Stability Questionnaire, a tool developed because of “outdated male/ female binary stereotypes.” Again synthetic sex trumps all. Death by cancer over detransitioning is acceptable as reported by the FTM patient who played the starring role in the study.
Tissue Engineering
The best explanation for the enthusiasm over make believe sex identities might be what the future holds. “Adventures in Baby-Making” discusses gender’s contributions to ART and the advent of family creation disjointed from traditional relationships and biological truth.
But there is more than this. Tissue engineering is being pursued for anatomical features likes breasts and genitalia. Consider that Brigham and Women’s Center for Transgender Health offers a “spectrum of gender firming surgical treatments” using “…the latest in 3D technology, tissue engineering and biomedical engineering…” This cult of synthetic science operates in the open in medical facilities across the country.
In 2022 a National Science Foundation Award was given to Rafaella De Vita, a Virginia Tech professor, for her study on the biomechanics of gender affirming surgeries (aka synthetic sex surgeries). De Vita’s specialty is female pelvic floor biometrics. She is a biomechanical engineer and the director of the university tissue engineering lab that goes by the acronym STRETCH. The article states, “De Vita will develop novel mathematical and computational models to capture both the similarities and differences between genitalia of those assigned male at birth and those assigned female at birth.” Her project collaborator is Dr. Cecile Ferrando who helped found the Cleveland Clinic transgender program, performed hundreds of “transitions” in her 5 years there, wrote a book about transgender “care,” and left to spread her insights at UCSD in 2024.
In tissue engineering synthetic scaffolds are created of biological material. The scaffolds are then either filled with fat or the body then replaces the scaffold with its own living tissue. This is in its infancy to date, but adds new meaning to synthetic sex docs like Joanna Olsen Kennedy who once claimed, “If you want breasts at a later point in life you can go and get them.” Tissue engineering, if safe and effective, might have merits for many applications. Altering biological truth for identity markets or transhumanist ventures are not among them.
Being verses Becoming
The 50s and 60s were a time of unrestrained expansion in science that speeds faster and faster by the day. Industry’s indulgence in synthetic sex identity markets began at Johns Hopkins when Howard Jones’ knife first cut into the flesh of a black man to create something his mind desired and a doctor and program deemed worthy. There were few patients then. Today there are hundreds of thousands, and they have their own acronym to boot. Medical racism might be the new apartheid but alongside race is now that new acronym, SOGI. A new class of people to abuse has been born.
Never mind that at conception a human is defined as male or female. Howard Jones once fought in court against this truth. No white coat assigns anything. They manipulate nature. “Gender” is the narrative. This is about becoming. It is about change and the evolution of man past states of being. Freeing humanity from the constraints of his God given flesh and blood is the dystopian vision. “Trans lives matter” only to the sciences for the prospects of a transhuman future. The rest are duped.
Author’s note: As I was rereading the Immortal Life of Henrietta Lacks, the Lacks family was in the news. An out of court settlement was made with Novartis who used the HeLa cell line without compensating the rightful owners, now the Lack’s estate. A previous settlement was made in 2023 with Thermo Fisher Scientific. More are pending.
Up Next
A coming post returns to Johns Hopkins and Howard Jones first synthetic sex patient, Phyllis Avon Wilson, to the culture of drag that has been cultivated in racial minority populations, and to an industry’s role in it all.
More like an era of mad science over patients.
Restacked, Mothers Grim. This is very excellent and well-researched. It deserves a high level of viewing.
Great pointing out of the intersection of cancer and the medicalized trans-identified person. The cancer industry is making their millions off of them.